- ICCONS,Shoranur, Palakkad (0466)2224869; 6238440945
- ICCONS, Pulayanarkotta,Trivandrum-11 (0471)2440232, 2447729
- icconssrr@gmail.com
- icconstvpm2018@gmail.com

ICCONS Recollection
INSTITUTE FOR COMMUNICATIVE & COGNITIVE NEUROSCIENCES TRIVANDRUM & SHORANUR SINCE 1998 IN THE SERVICE OF MANKIND WITH DIFFERENTIAL ABILITIES AND NON COMMUNICABLE NEUROLOGICAL DISORDERS
THE CONCEPT AND SCIENTIFIC PERSPECTIVES
Necessity is the mother of invention. The need to set up an Institute for Rehabilitation of speech, language and cognitive disorders was also evolved out of “necessity”. The World today is undergoing a rapid transition and transformation of its demographic pattern. There is an overall increase in life expectancy as we could effectively conquer many infectious and contagious diseases. Education and Cultural development have paved way to high standard of living. Environmental sanitation and better housing increase in leisure time, technological and scientific advancement, above all, awareness about health and diseases have all got a direct impact on our state of health life expectancy. Maternal and Reproductive health, Infant supportive care, Scientific approach to child development, Immunizations programs have made perceptible impact on family size and reduction in infant mortality. Most developed countries are in the stage IV of DTM while most developing countries are in the Stage II or Stage –III. The waves of demographic transition have its impact on many parts of India, Kerala is very rapidly moving to the stage-IV of DTM.
DTM has a direct impact on the health status and pattern of various disorders and disabilities prevailing on a country.
THE ICIDH –WHO FRAME WORK FOR MANAGEMENT OF DISABILITIESThe approach to management of disabilities, which was earlier confined to rehabilitation institutions, has found its way as a continuum from acute care hospitals to chronic care hospitals. The protocol and principle of current management and rehabilitation is based on the WHO principle of ICIDH : International Classification of Impairments, Disabilities, and Handicaps. These concepts, however, has not gained much attention in the health care policies of many developing countries including India.
The WHO framework towards the classification and management of disabilities – The ICIDH was proposed in 1980 and later revised in ICDIH-2 in 2001. The frame work is formulated on the basis of the evolution of disabilities leading to handicap from a state of health through the interaction of different agents of physical, biological and chemical nature as well as the environment with the individual. This frame work, a linear one also provides the opportunity to prevent, ameliorate the severity of a disabilities resulting from disease state or even may reverse the situation through appropriate intervention at each stage.
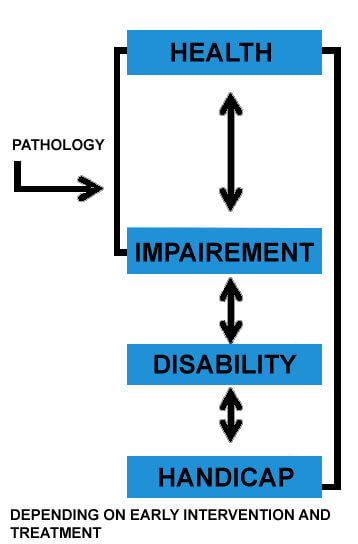
The impairment may lead to disability of permanent or partial nature that may be reversible or irreversible. The disability ultimately decides the handicap the person is going to have based on social and environmental factors.
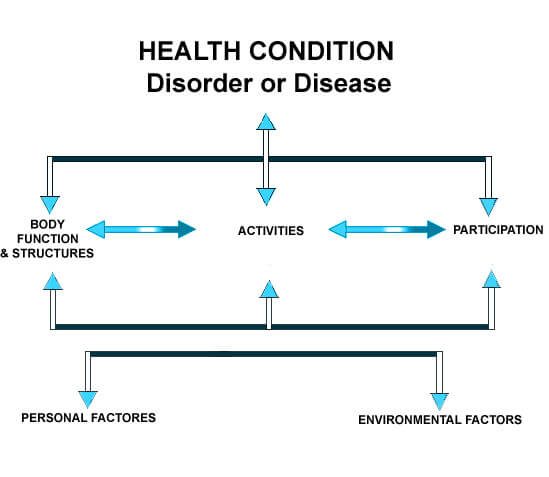
The latest approach, International Classification of Functioning, Disability and Health, known as ICF, is to provide a unified and standard language and framework for the description of health and health-related states. The program considers the change from a state of health or well being to impairment of function caused by specific pathology due to different causes. The ICF is a framework for organizing and documenting information on functioning disabilities and conceptualize functioning as a dynamic interaction between environmental factors and personal factors. The ICF classification also provides room for planning research and even environmental changes to make a person’s life comfortable and happy.
ICF provides a standard language and conceptual basis for the definition and measurement of disability, and it provides classifications and codes. It integrates the major models of disability - the medical model and the social model - as a “bio-psycho-social synthesis”. It recognizes the role of environmental factors in the creation of disability, as well as the role of health conditions.
The WHO in its endeavor to provide “Health for All” in the 21st century sensed a need for change in the perspective towards health and disease-“a shift of focus from communicable disorders to non -communicable disorders”. The disorders under this category include developmental disabilities/disorders (Mental Retardation, Autism, Cerebral Palsy, Learning Disability, congenital hearing loss, congenital blindness), genetic and metabolic disorders, neurological disorders like stroke, Parkinson’s disease, motor neuron disease, dementia, heart diseases, cancer, complications of accidents and injury and also AIDS and its complications. The list is so exhaustive, yet incomplete. Many of the disorders are a leading cause for various types of disabilities.
The WHO also reports that about 10% of the world population (an estimated 600 million people) experience one or other form of disabilities and more so in poor countries where basic amenities itself is a challenge. A large proportion of the disabled people are in the WHO’s South East Asia region. The Global Burden of Disease reports five out of ten most disabling disorders in the world are developmental in nature. In addition to this neurological disorders leading to disabilities, malnutrition, AIDS and mental disorders are increasing in its prevalence.
World Federation of Neurology (WFN) and WHO in their combined study of 1999, revealed that the second most common cause for death is neurological disorders and out of every nine deaths in the world, one is due to a neurological problem. Because of the incomplete and unscientific way of reporting the prevalence, it is often reported erroneously low. Therefore it is imperative on the part of any civilized society to provide appropriate measures for the management and rehabilitation of these individuals to minimize the impact of the disabilities and handicap and bring them to the front of life.
Disabilities as a whole and specifically that affecting higher mental functions such as learning, memory, intelligence, language and other cognitive abilities received little attention in the general realms of Clinical Medicine, General Pediatrics or even in the General Neurology Practice. Technological development like advent in computer science, the recent concepts in Neuroimaging, the genome project and research progress in molecular genetics and metabolism have improved our understanding of many developmental, genetic and metabolic disorders.
The plight of communicatively and cognitively impaired individuals demands special attention. Since the faculties of speech, language and cognition have unique interfaces in many human activities and social life. These disorders also demand multi disciplinary interventions at multi- functional level. Unfortunately till to date, there is not a single organization in our country that champions their cause.
The Government of India has taken many steps for the welfare of the disabled, but these measures generally been geared to meet the needs of certain selected group of disabilities such as congenital hearing loss, visual impairment or physical disabilities by providing of appliances, social rehabilitation or job placement. However selective individual measures for early detection and prevention of these disorders and exploring the application of modern technological and technical advancement for their management are lacking. Persons with cognitive and communicative disorders of developmental or acquired nature such as learning disability, autism, mental retardation, cerebral palsy, multiple congenital anomalies, acquired aphasias; dementia, traumatic brain injury and many other neuro-degenerative disorders have received little attention in this regard. Scientists and health policy makers can no longer ignore to address this important issue, because the problems associated with these conditions that are central to the health and well being of vast number of people. These disorders should be recognized as key challenges to public health and be granted new priority among other conditions concerned with human disabilities and handicaps.
Compared to many developing nations of Asia, India especially, Kerala is having demographic transition pattern and health indices similar to that of the most developed countries of the world. Over the past 50 years the country has made unprecedented gains in health front by reducing infant and maternal mortality and increasing life expectancy. Yet there is an unforeseen increase in the prevalence of children and adult with various developmental and acquired disabilities leading to morbidity and mortality.
The advancement in life supporting measures, technological and technical progress, life style changes have indirectly contributed to the increasing morbidity by bringing forth to life many infants with various developmental disabilities. The nation is not yet fully equipped to manage the mounting number of disabilities and non communicable neurological disorders in terms of expert manpower, technological support and Research & Development.
It is against this backdrop, that “Institute for Communicative and Cognitive Neurosciences”, first of its kind in India, has been established in Kerala, a state which has many firsts to its credit in the field of health.
The project of SRCCD to establish ICCONS was proposed in the framework of ICIDH developed by WHO and modified and updated with that of ICF for the management of disabilities and Non Communicable Neurological Disorders. In accordance with this framework, the Institute conceptualize its programs and activities for treatment, rehabilitation and Research & development. Accordingly, all disabilities have to be investigated to find out its cause and treated appropriately wherever possible. Rehabilitation program should be planned according to the age, sex, type and severity of the functional impairment. Systematic evaluation is required in each case to make a full diagnosis to assess the functional abilities and deficits according to International standards. This helps in setting specific goals for education, vocational placement and long term independence within a reasonable time period. This program requires the interaction and combined effort of a multidisciplinary team in which the Neurologist is the team leader and other medical and paramedical forces, which include Pediatrician, Orthopedician, ENT Specialist, Psychiatrist, Physiatrist, Speech Language Pathologist, Clinical Psychologist, Clinical Linguists, Physiotherapist, Occupational therapist, Special Educators, Sociologists and Vocational experts are members of the team.
The planning for Children with disabilities should look into what is the possible Educational placement for them and the expected out come by the time they are adults. Special Education of Residential type is ideal for them. The theme of the special education should be a curriculum based one with a prospective plan and long term goals so that gradual Integration to the main stream education is achieved.
The development of any disability and its nature should be anticipated in the event of any health compromising conditions whether social, environmental, developmental disease related or person related. Hence the slogan of early detection and prevention.
The disability should be prevented and early detection is a scientific research before its development rather than identifying the condition once it is set in.
ICCONS VIEWS
- Hereditary, familial and genetic disorders requires anticipation and premarital counseling through scientific pedigree analysis.
- Target individuals and individuals at risk may be identified by genomic scan.
- Developmental disabilities.
- Proper obstetric care should be given in the antenatal period, peri natal period and post natal period to avoid birth injuries, hypothec ischemic encephalopathies.
- High risk mother and high risk infants should be identified and properly followed up.
- Acute phase of diseases should be managed appropriately to minimize chronic disabilities such as strokes, head injuries, brain tumors etc.
- Rehabilitation is multidisciplinary early language and cognitive intervention.
- Early rehabilitation for visually and physically handicapped.
- Appropriate educational planning and educational programming.
- Reduction of environmental barriers.
- Vocational training and job placing.
- Social environment to develop personality.